
Your patients deserve better than a call center.
A transparent comparison of HPM, Ruby, Ginger Phone, Ginger Desk, and in-house staffing
from the perspective of a small holistic healthcare practice.
Most practitioners are not actually choosing between “phone plans.”
They are choosing how they want patients to experience their practice.
The real question is not:
“Who can answer the phone cheapest?”
The real question is:
"Who can help patients feel taken care of while allowing the practitioner to stay focused clinically?"
WHAT PRACTITIONERS USUALLY DISCOVER TOO LATE
Most patients are not calling just to “schedule.”
They are often calling:
in pain
confused
overwhelmed
after feeling dismissed somewhere else
trying to decide whether they can trust the practice
That means the front desk is not just an administrative role.
It becomes part of the patient experience.
At the same time, many small practices are trying to balance:
callbacks
scheduling
patient communication
EMR work
supplement coordination
labs and follow-up
operational loose ends
while still trying to stay present clinically
.
That operational overload is usually the real issue.

TRANSPARENT PRICING COMPARISON
Most pricing pages make comparisons difficult.
We prefer to show the actual structure so practitioners can evaluate tradeoffs honestly.
| Service | Approximate Effective Cost | Pricing Structure | Operational Scope |
|---|---|---|---|
| Ruby | $3.45–5.00 /min | Bundled monthly phone-minute packages | Call center with hundreds of callers answering for every client. |
| Ginger Phone | $2.60–4.30 /min effective rate depending on package | Tiered bundled phone plans | Package-based phone answering and scheduling. |
| Ginger Desk | $1,999 to $3,499 /month | Administrative support layer separate from scheduling | Operational/admin workflows |
| In-house receptionist | $3,000 to $6,500 /month true employer cost | Fixed payroll overhead | Deep continuity + full operational flexibility |
| HPM | $2.13 /min reception $1.63/min admin $0.40/min project work $249 startup fee Usually $300 to $1,500 per month depending on needs and clinic volume |
Flexible blended utilization | Phones + admin + EMR + operational support |
Examples by clinic size
Here is a cost comparison based on clinic size:
| Practice Size | HPM | Ruby | Ginger | HPM Savings |
|---|---|---|---|---|
| Small Practice | $300 | $395 | $769 | $95–$469/mo |
| Medium Practice | $700 | $1,050 | $1,299 | $350–$599/mo |
| Busy Solo Practice No Front Desk |
$1,500 | $2,300 | $2,199 | $699–$800/mo |
For many small practices, the biggest difference is not simply cost per minute.
It is whether the system can flex between patient communication and operational work without requiring multiple disconnected vendors or a full in-house staffing structure.
WHAT ARE YOU ACTUALLY COMPARING?
| Option | Typical Strength | Common Limitation |
|---|---|---|
| Traditional answering service | Simple overflow call coverage | Support comes from a broad rotating team, which can make continuity and practice familiarity harder to build. |
| Ruby | Polished phone answering | Primarily phone coverage; little admin or EMR support, and support comes from a broad rotating team, which can make continuity and practice familiarity harder to build. |
| Ginger Phone | Small teams and structured phone-answering packages | Separate from deeper operational/admin workflows |
| Ginger Desk | More operational support | Starts around $1,999/month and operates as service layer separate from and in addition to reception services |
| In-house receptionist | Deep continuity | High fixed overhead and management burden |
| HPM | One team that can flex between phones, admin, EMR, and operational support | Requires onboarding and relationship-building like any real team member |
How HPM actually works
HPM was built around a simple idea:
Small healthcare practices often need more than a traditional answering service, but are not ready for the complexity and fixed overhead of building a full in-house front office team.
So instead of separating:
phone answering
admin support
EMR work
patient communication
operational follow-up
into different systems or vendors, HPM was designed to function more like an extension of the practice itself.
A blended support model
Depending on the needs of the practice, HPM teams may help with:
patient communication
scheduling
callbacks
EMR workflows
supplement coordination
labs and follow-up
inbox/admin tasks
operational support
The goal is not simply to “cover phones.”
The goal is to help the practice operate more smoothly while protecting the practitioner’s ability to stay focused clinically.
Continuity matters
Most practices do not want a random rotating call-center model.
They want support that:
learns the practice
understands patient communication style
becomes familiar with workflows
builds trust over time
That onboarding process usually takes approximately 2–4 weeks, similar to training any real team member.
Flexible utilization instead of rigid staffing
Many systems separate:
phone answering
admin work
operational support
into separate products, teams, or pricing structures.
HPM was designed differently.
The same team can often move fluidly between patient communication and operational work depending on what the practice actually needs that day.
That flexibility is one of the main reasons many small practices continue using HPM even after hiring internally.

The first voice a patient hears is already part of the care.
Dr. Sam Schikowitz
Founder, Holistic Practice Management
Why I built HPM
In 2006 I needed a receptionist for my small practice.
I built HPM because I experienced firsthand how difficult it was to be both practitioner and front desk at the same time.
I would finish patient visits and still be mentally tracking:
callbacks
voicemails
scheduling
paperwork
operational loose ends
At first, I thought the issue was simply answering the phone.
What I eventually realized was that patient communication shapes trust before the first appointment ever happens.
Ruby
Ruby is a polished answering-service platform structured around monthly bundled phone-minute plans.
This is a call center, and your patients will be talking with a different person every time they call.
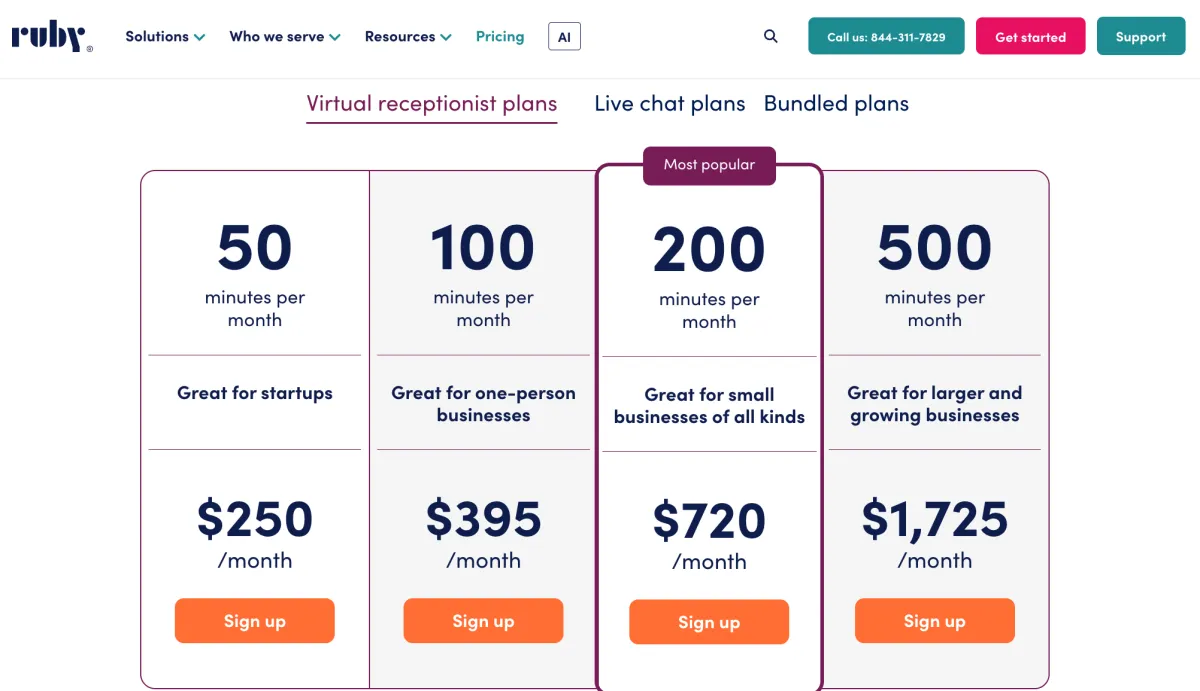
| Ruby Plan | Monthly Cost | Included Minutes | Effective Rate |
|---|---|---|---|
| Starter | $250 | 50 minutes | $5.00/min |
| Basic | $395 | 100 minutes | $3.95/min |
| Essential | $720 | 200 minutes | $3.60/min |
| Growth | $1,725 | 500 minutes | $3.45/min |
Ruby pricing as of April 2026.
Actual price per minute will typically be higher if you are not using the complete bundle.
Ruby can work well for practices needing traditional call answering coverage, but many practitioners still find themselves separately managing:
callbacks
EMR work
patient follow-up
scheduling coordination
operational admin
Ginger Phone
Ginger Phone is structured around bundled monthly phone-minute packages.
You receive dedicated 2 US based team members who answer phones, answer basic questions, and schedule patients, but do not do administrative work.
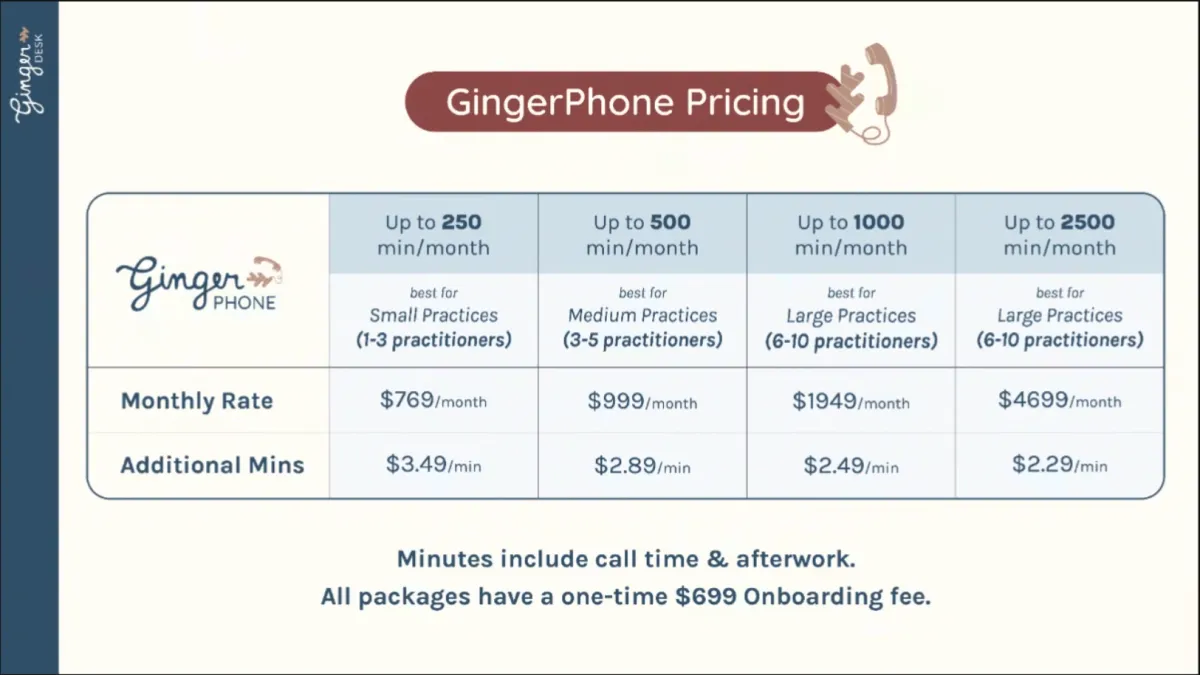
| Ginger Phone Plan | Monthly Cost | Included Minutes | Approx. Effective Rate |
|---|---|---|---|
| Starter | $769 | 180 minutes | ~$4.27/min |
| Growth | $1,299 | 360 minutes | ~$3.61/min |
| Professional | $2,199 | 720 minutes | ~$3.05/min |
| Enterprise | $4,699 | 1,800 minutes | ~$2.61/min |
Ginger Phone pricing as of April 2026. Packages range from $769/month to $4,699/month depending on included minutes and practice size.
Notes
minutes include call time and afterwork
additional minutes billed separately
separate onboarding fee
focused primarily on phone-answering coverage
deeper operational/admin support handled separately through Ginger Desk
Ginger Desk
Ginger Desk is a separate operational support layer focused on inbox management, booking workflows, document support, coverage VA support, and clinic coordination.
Ginger Desk staff handle each client's admin work twice per day.

Ginger Desk pricing as of April 2026. Plans begin around $1,999/month and scale upward depending on workflow complexity and volume.
Notes
separate pricing structure from Ginger Phone
more operationally involved than standard answering services
pricing rises significantly as practices rely more heavily on operational support
structured package model rather than flexible blended utilization
In-House Receptionist
Hiring an in-house receptionist can absolutely work well for some practices.
A great front desk person can become deeply woven into the culture and rhythm of a clinic.
But many small practitioners underestimate how much operational responsibility comes with becoming an employer.
The hourly wage is usually only the beginning.
| Base Wage | Approximate Real Employer Cost | Part-Time Monthly Cost (~20 hrs/week) |
Full-Time Monthly Cost (~40 hrs/week) |
|---|---|---|---|
| $16/hr | ~$20–23/hr | ~$1,700–2,000/month | ~$3,500–4,000/month |
| $20/hr | ~$25–29/hr | ~$2,100–2,500/month | ~$4,300–5,000/month |
| $25/hr | ~$31–36/hr | ~$2,700–3,100/month | ~$5,300–6,200/month |
*Approximate employer cost may include
payroll taxes,
unemployment insurance,
paid downtime,
software/accounts,
training time,
management overhead, and
operational coverage gaps.
Actual costs vary by state and staffing structure.
What practitioners often underestimate
Most practitioners are not just hiring support.
They are also taking on responsibility for:
recruiting
interviewing
onboarding
training
supervision
payroll systems
state employment tax agencies
unemployment insurance
scheduling coverage
sick days
vacations
disciplinary conversations
turnover
continuity risk when someone leaves
And when your one front desk person is unavailable, the phones often still roll to voicemail.
That’s not a criticism of employees.
It’s simply the operational reality of small practices.
The challenge is continuity
The challenge is not just finding someone kind and capable.
The challenge is building reliable operational continuity around one human being.
When only one person knows:
workflows
patient communication patterns
scheduling systems
EMR processes
operational details
even normal life events can create disruption:
illness
vacations
maternity leave
burnout
unexpected resignation
rapid practice growth
Why some practices continue using HPM even after hiring
Some practices initially use HPM because they are not ready to hire in-house staff.
Others continue using HPM even after building an internal team.
Why?
Because operational continuity becomes increasingly important as the practice grows.
The goal is not to eliminate human staff.
The goal is to prevent the entire patient communication system from depending on a single human being.
HPM pricing
| Support Type | Current Pricing |
|---|---|
| Reception Support | $2.13/min |
| Administrative Support | $1.62/min |
| Project Work | $0.40/min |
| Monthly Phone + Readiness Fee | $79/month |
| Startup Fee | $249 |
| Reception Billing Minimum | 3-minute minimum per call |
Typical monthly range
Most solo practices spend approximately:
$300–$1,500/month
depending on:
patient volume
call frequency
scheduling complexity
EMR/admin workload
communication needs
Larger or multi-provider practices may range higher depending on scope.
Real-world examples
What HPM support can include:
| Practice Example | Practice Size | Typical HPM Support | Approximate Monthly Cost | Typical Outcome |
|---|---|---|---|---|
| Solo Startup Practice |
1 practitioner 8–15 patients/week |
|
$300–500 /month | HPM is handling every incoming call and the Practitioner is avoiding the overhead of hiring in-house staff too early. |
| Established Solo Holistic Practice |
1 practitioner 20–35 patients /week |
|
$700–1,500 /month | Thorough coverage of basic front and back office tasks. |
| Growing Multi-Provider Clinic |
2–4 practitioners Higher patient volume + operational complexity |
|
$2,000–4,500 /month | Allows the practice to scale operationally without relying entirely on one in-house staff member. |
| Hybrid In-House + HPM Model |
Internal front desk staff + HPM continuity layer |
|
Cost varies depending on the duties HPM undertakes, and can be flexible based on need. | Reduces operational fragility and continuity risk during staffing transitions, growth periods, or coverage gaps. |
The difference most practitioners miss
Many systems separate:
phone answering
admin support
EMR work
operational follow-up
into different people, products, or pricing structures.
HPM was designed differently.
Our teams can often move fluidly between:
patient communication
scheduling
EMR work
supplement coordination
labs and follow-up
operational admin
depending on what the practice actually needs that day.
That flexibility is difficult to achieve with traditional answering services and often much more expensive to achieve with full in-house staffing.
What practitioners are actually buying
One of the most common things we hear is:
“It feels like they’re actually part of the practice.”
That difference matters more than most people expect.
Patients can feel when communication is transactional rather than connected to the practice.
Practitioners often think they are buying:
phone answering
scheduling help
callback coverage
But what they are usually trying to solve is:
constant interruption
delayed callbacks
fragmented communication
operational overload
missed referral opportunities
inability to stay focused clinically
patient trust gaps
Who HPM is best suited for
HPM is often a strong fit for:
solo practitioners
growing holistic practices
practices overwhelmed by callbacks and operational fragmentation
practitioners wanting continuity without hiring full in-house staff
practices that value patient trust and communication quality
practitioners who want support that learns the practice over time
HPM may NOT be the best fit if:
you only need basic call answering and scheduling
you want every call answered within a few rings, even if by a different person each time
you want night and weekend coverage
continuity and practice familiarity are not priorities
Curious what this could look like for your practice?
We offer a 30 day risk free trial. If you don't like the service after 30 days, you walk away without any cost.
HPM offers a more flexible and operationally complete alternative to answering services or full in-house staffing alone.
So if you simply want:
fewer interruptions
better patient communication
more continuity
less operational overload
more ability to stay focused clinically
We’re happy to talk through your current setup and whether HPM would actually make sense for your practice.
FAQ
Do I get the same people over time?
Yes! Continuity is a major part of how HPM works.
Most practices work with the same core team over time so the people answering the phone learn the practice, the patients, the workflows, and the tone of communication.
That consistency is important. Patients often end up recognizing and building trust with the receptionist supporting the practice.
HPM is not structured like a rotating call-center pool.
If your team is unable to cover, such as illness, we will find and train temporary replacements.
We do reserve the right to move clients to a new team if we are sure the client will get better service there.
What counts as reception vs admin vs project work?
Reception support generally includes live phone answering, scheduling, callbacks, patient communication, and front-desk workflow coordination.
Administrative support includes work done between calls inside the operational flow of the practice: things like EMR updates, portal coordination, labs, supplement coordination, paperwork follow-up, and scheduling workflows.
Project work is lower-urgency operational work that can often be completed asynchronously by team members outside the live reception flow.
The exact mix varies by practice.
Can HPM work alongside in-house staff?
Yes. Many practices use HPM as part of a hybrid model.
Sometimes HPM handles overflow calls, callback support, operational continuity, or coverage during vacations, sick days, staffing transitions, or growth periods.
Other practices start with HPM before hiring internally, then keep HPM as a continuity and operational support layer afterward.
One of the biggest operational risks for small practices is becoming completely dependent on a single front-desk employee.
What happens if volume changes month to month?
HPM was intentionally designed to flex with smaller practices.
Some months are busier than others. Practices add providers, launch services, go on vacation, experience staffing transitions, or hit seasonal fluctuations.
Because HPM is usage-based rather than a rigid staffing package, support can usually scale up or down much more easily than traditional in-house hiring.
How long does onboarding take?
Most practices take about 2-4 weeks to fully onboard.
The goal is not just to “answer phones.” The team needs to learn the practice itself: scheduling flow, patient communication style, EMR workflows, provider preferences, boundaries, supplements, labs, escalation rules, and operational rhythms.
In many ways, onboarding looks more like training a real front-desk team member than activating a generic answering service.
Do you offer holiday, after-hours, or weekend coverage?
We have offered this option to our clients over the years, but the answer has been: No, this is not actually worth the increase in cost. It is possible to configure our phone system to route calls to a 3rd party call center after hours and on weekends and holidays. If this is important to you, let us know and we can discuss how we can make this work.
